We need to optimise how funds for eye health are spent so we can make the most impact.
Understanding exactly how to get ‘more eye health for the money’ is critical, along with need, sustainability, affordability, and feasibility. Unfortunately, evidence on how to do this is very limited.
The Lancet Global Health Commission on Global Eye Health1 undertook a comprehensive eye health economic literature review of the cost-effectiveness of eye health treatments. This highlighted the scarcity of cost-effectiveness data, particularly for low- and middle-income countries (LMICs). It also showed that there is significant variation in the way cost-effectiveness studies are conducted.
The commission identified 182 reports of cost-effectiveness of interventions for 16 ophthalmic conditions. The most frequently studied interventions addressed age-related macular degeneration, glaucoma cataract and diabetic retinopathy, however the commission focussed on the most significant causes of vision loss globally – cataract and uncorrected refractive error.
Cost-effectiveness of cataract surgery
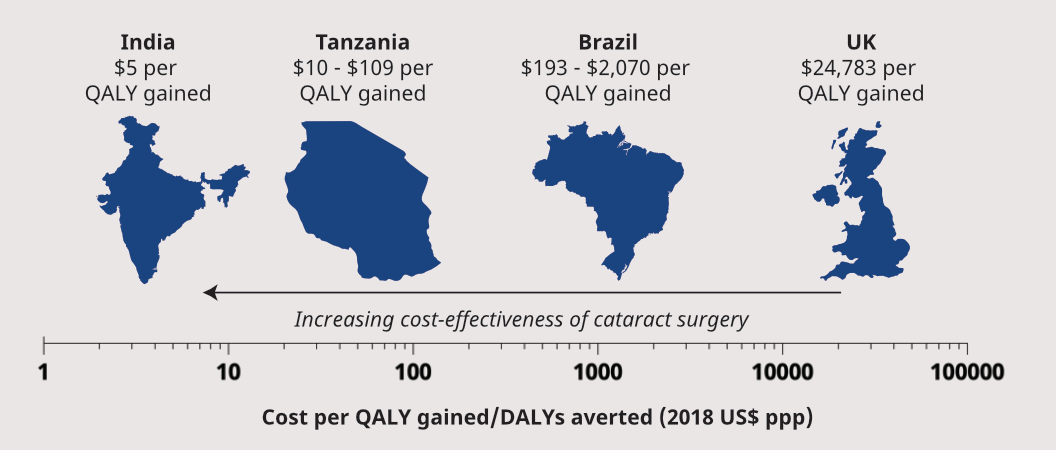
The Commission reviewed the cost-effectiveness of cataract surgery (Figure 1). The review was comprised of 11 studies that provided 58 national or regional estimates,
Health benefits that were reported as:
Disability Adjusted Life Years (DALYs): measures the overall burden of disease by counting the overall number of years lived with a disability. One DALY is equal to one year of health life lost.
Quality Adjusted Life Years (QALYs): quantifies the health effect of an intervention or prevention program.
Figure 1: Indicative cost-effectiveness ratios for cataract surgery
Key findings:
Cataract surgery tends to be more cost-effective in LMICs.
This might partly be because people in higher income settings receive surgery for more mild vision loss. It may also be due to the higher remuneration of eye care professionals in higher income countries.
The large majority of studies reported costs per QALY gained or DALY averted less than $1,000.
Cost effectiveness of screening/treating uncorrected refractive errors
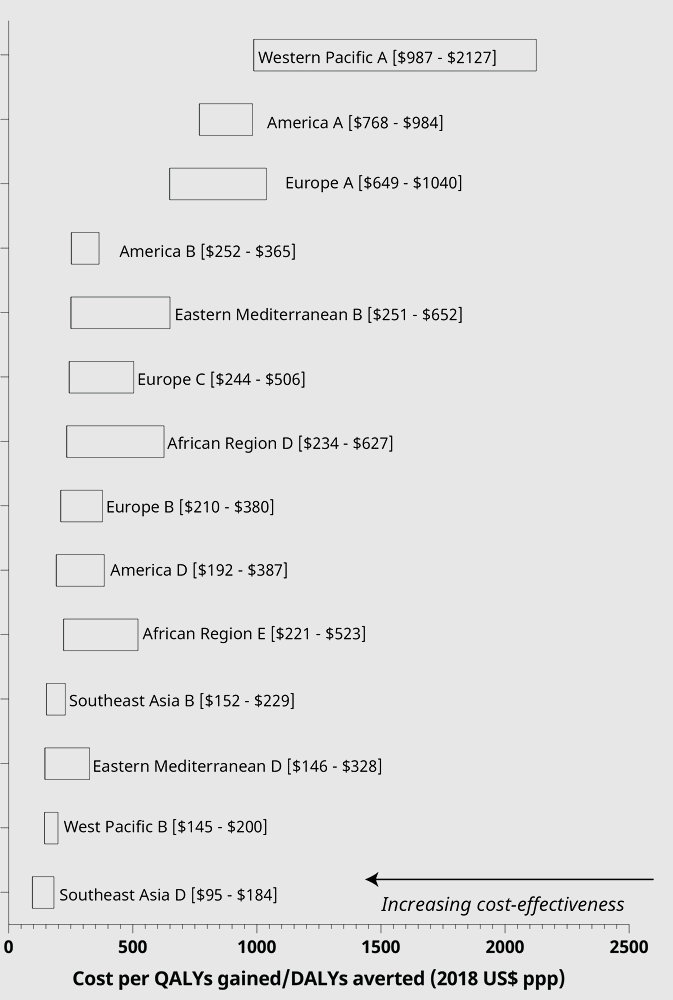
The Commission identified 3 large studies that examined the cost-effectiveness of screening or treating uncorrected refractive errors in children in schools or in facilities. These studies included 16 national or regional estimates. Figure 2 shows the reported cost-effectiveness ratios for WHO sub-regions.
Figure 2: Indicative cost-effectiveness ratios for cataract surgery (by WHO subregion)
Key findings:
The most cost-effective strategy in all 14 regions involved screening children in the 11-15 year age group ($95), compared to other age groups. [Frick, 2009]
Screening and treating school children in India is more cost-effective in urban areas ($264) compared to rural areas ($1448).
There is a need for strengthened evidence
More consistency
The wide variation in study methodologies results in research that is very difficult to compare. Particularly due to the differences in:
Costs included
How health benefits are measured
Surgical procedure
Assumed duration of the benefit of the eye health service.
Recommendations from the Commission:
There is a need for substantially more economic data to inform countries deciding which eye health services to offer within UHC.
There is also the need for more cost-effectiveness data to inform decisions relative to other health priorities.
Data are particularly limited from LMICs, a gap that must be urgently addressed to better inform policy and planning decisions.
More cost-effectiveness, budgetary impact and feasibility analyses are needed from a broader range of settings to better inform national decision-making.
Cost and cost-effectiveness analyses evaluating alternative service delivery approaches should be undertaken.
For example, moving to greater primary and community-based delivery platforms, integration with other services and task sharing. Extended cost-effectiveness analyses are needed that include health system objectives such as improved financial protection and equity to inform policy and planning decisions.
Burton, M., Ramke, J., Marques, A., Bourne, R., Congdon, N., Jones, I. et al. Lancet Global Health Commission on Global Eye Health: Vision Beyond 2020. The Lancet Global Health (2021).