Join the Leading Global Eye Health Alliance.
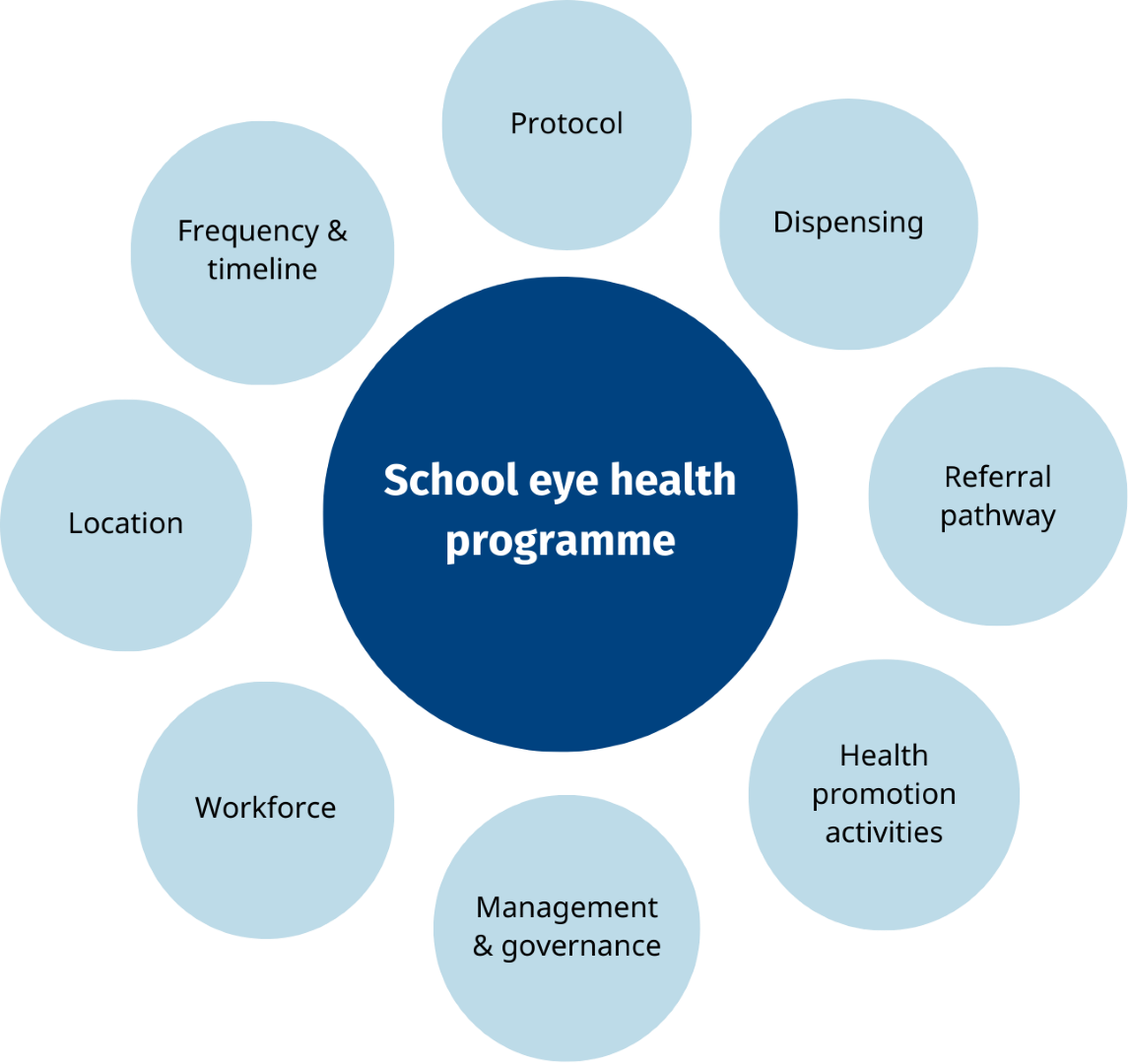
MembershipOnce the goals and objectives of the programme have been clearly stated, it is time to reflect on the activities and operational procedures of the programme. Evidence-based protocols should be chosen based on available personnel (eg WHO screening implementation guidelines, REACH, WCO Paediatric resource).
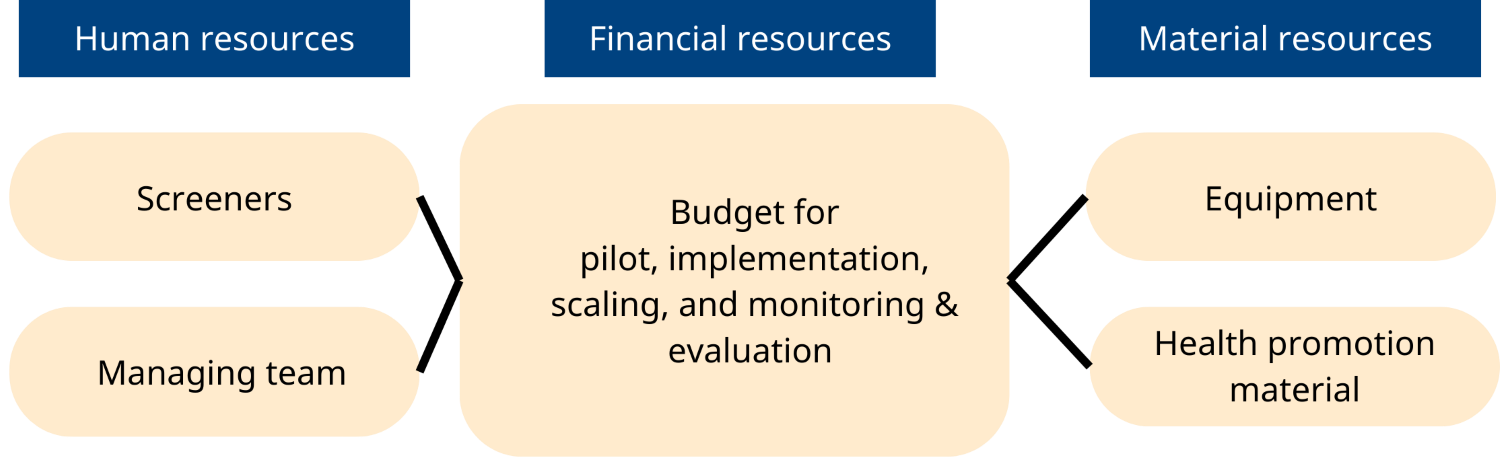
Based on the previous steps, resources should be estimated for each component of the programme.
The design of your school health intervention will impact the materials and resources required, the training needs and human resources and the extent of service provision being offered during different phases of the program. For example, an integrated screening day may include screening and some basic provision of services such as glasses as well as referral but a school eye health program may only include the delivery of eye health awareness by teachers and basic screening, with children referred to trained services if needed.









