





Join a powerful, unprecedented alliance for better eye health for all.
Join IAPB-
Choose an alternate language here

WHO and IAPB answer questions which were raised in the WHA 75 session on “Universal Health Coverage and Eye Health: Promoting Country Action.” The session launched the new suite of WHO tools along with a panel discussion on Integrated people centred eye care.
Although the tools are designed to be applicable to any country, in reality, the primary audiences are more likely to be governments of low- and middle-income countries and the agencies working with them. The proposed “Analyse-Plan-Do-Review” cycle outlined in the Guide for action document is in line with best-practice health services planning and management around the world, regardless of the socio-economic setting. The very message at the heart of the tools, i.e., eye care that is people-centred and integrated, is relevant to any country. Also, the tools are designed in a modular way so that countries may select components for planning and implementation or monitoring of eye care, in line with the actual need.
The ECSAT covers some aspects of integration of eye care within national disaster preparation planning. However, migrant populations do not feature as a specific focus. We feel that this is a complex, and most certainly important, issue that requires a separate and more in-depth approach (or tool) than would have been able to be covered in the current ECSAT.
In order to avoid doubling up of information and to ensure government engagement from the beginning of ECSAT implementation, the tool is available by request from WHO. By making it freely downloadable, without the necessary engagement of WHO and other relevant stakeholders in country, we feel that there is a risk of poor coordination and lack of information translation into planning. WHO is happy to share the tool with any organization as part of a wider planning exercise in collaboration with the governments. Regarding the indicator data, the creation of an eye care monitoring framework is intended to be driven by governments, primarily by eye care planners and policymakers in the Ministry of Health. The Ministry of Health should be responsible for collecting and reporting of the eye care indicators data.
To ensure that IPEC policies and plans include children, it should be coordinated and developed collaboratively across sectors that involve children (such as education or social services). The linkages between eye care services in relevant programmes (such as maternal and child health or school eye health) should also be reinforced. Engaging the sector/programmes representatives and planners, as well as other relevant stakeholders, allows the development of more comprehensive and inclusive plans and policies.
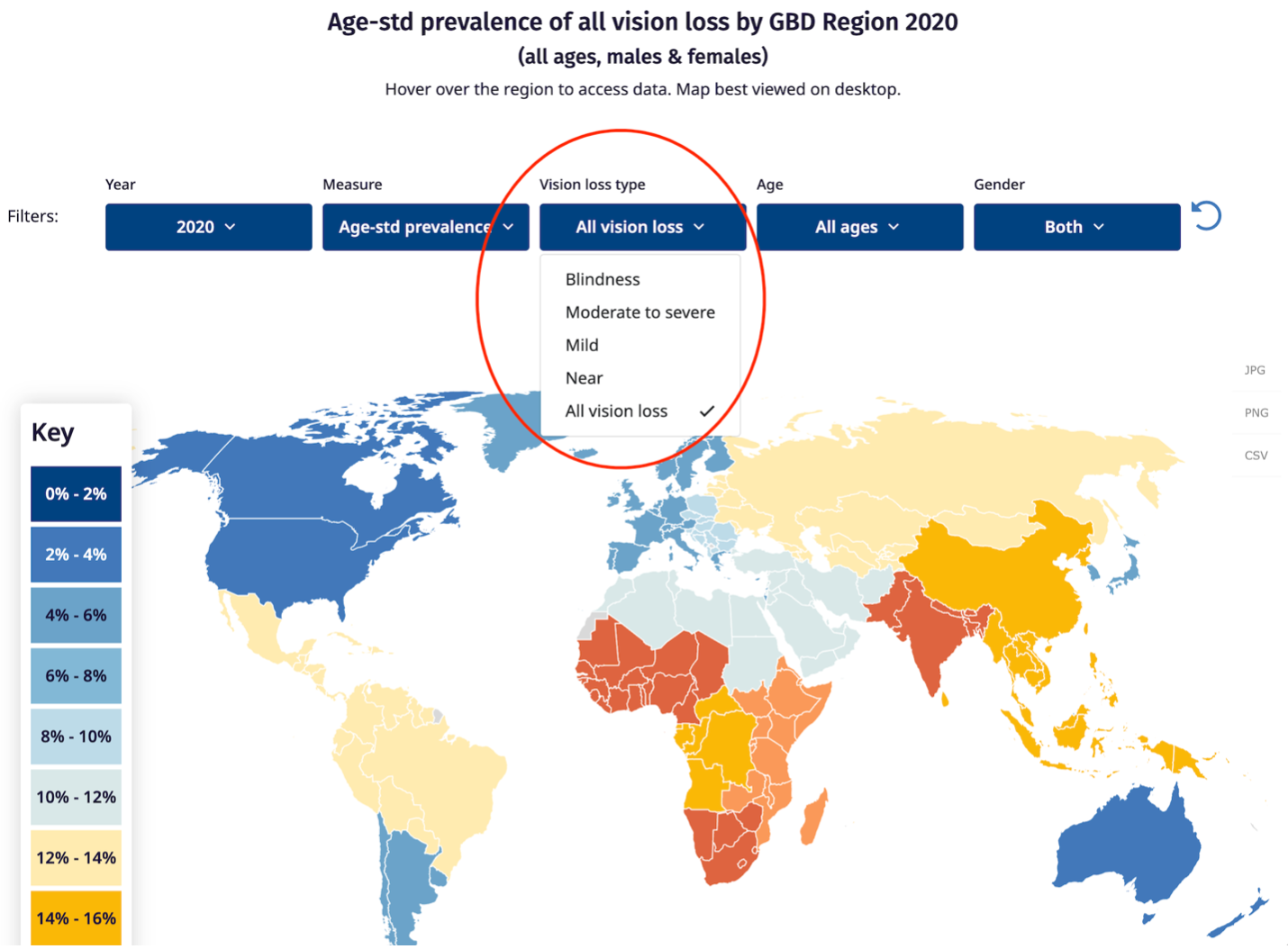
The IAPB vision atlas shows statistics on blindness and vision impairment disaggregated by regionas and countries. Please visit https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/gbd-regions/ for the data on blindness and vision impairment by global burden of disease sub- regions; and https://www.iapb.org/learn/vision-atlas/magnitude-and-projections/countries/ for countries. The drop down allows users to select the options that they would like.
The learnings from implementation of IPEC in one country can obviously be helpful in other country settings. Please share your country experience on implementation of IPEC to IAPB by writing an email to: [email protected] IAPB will share such experience in the form of country case stories. Please visit the Integrated People-centred Eye Care Advocacy to Action Toolkit. The chapter on advocacy approach for IPEC (specifically 5.4 Communicating the outcomes) will be helpful in sharing your country experience to us.
With special thanks to Jessica Thompson, Stuart Keel, Vera Carneiro & Anthea Burnett


















