Join a powerful, unprecedented alliance for better eye health for all.
Join IAPB-
Choose an alternate language here

The COVID-19 pandemic presented challenges when it came to continuing glaucoma care. Our routine practice had to be modified. Most of the patients who need glaucoma care are in the elderly age group and at high risk of contracting COVID-19. We had to develop new guidelines for optimum care, at the same time minimizing the spread of the virus. Since most of our examinations require close contact with the patients, we needed more protection than what the standard PPE could provide.
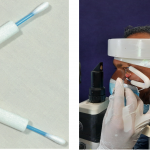
The commonly available slit lamp breath shield was not enough to provide sufficient protection from aerosols generated from patient’s breath. Hence, we experimented and developed a novel broader slit lamp breath shield which gave complete protection. It was also convenient to do routine tests such as applanation tonometry and gonioscopy trouble free. (Image 1)
 Separating the patient eyelids for complete eye examination was a challenge. An innovative 3D printed lid separating device called iOpener was developed and found very useful not only for eye examination but also for certain OPD procedures like applanation tonometry, Bleb needling etc.,(Image 2)
Separating the patient eyelids for complete eye examination was a challenge. An innovative 3D printed lid separating device called iOpener was developed and found very useful not only for eye examination but also for certain OPD procedures like applanation tonometry, Bleb needling etc.,(Image 2)
To reduce patient waiting time within the clinic we started using non-mydriatic fundus photography especially for stable glaucoma patients. The fundus images were uploaded into the electronic medical records so that the physician can view them in their monitor within their cubicle saving significant waiting time. 
Visual field testing is an inseparable part of glaucoma care. But there were no proper sanitizing guidelines for using standard Humphrey perimetry during the pandemic. Hence, we shifted to clinically validated virtual reality based portable perimetry testing( C3FA – C3 Field Analyzer) (Image 4). C3FA was conceptualized, engineered, developed and validated with standard perimetry in our clinic which is now commercially available.
 Frequent cleaning of Optical coherence tomography machine lens between patients was a challenge since alcohol in the sanitizing solution can damage the coating on the lens. A convenient way to protect the lens is to cover the lens with thin plastic wrap (Ezee Wrap) which is commonly used for packaging. This not only protects the lens but is also easy to clean and replace.
Frequent cleaning of Optical coherence tomography machine lens between patients was a challenge since alcohol in the sanitizing solution can damage the coating on the lens. A convenient way to protect the lens is to cover the lens with thin plastic wrap (Ezee Wrap) which is commonly used for packaging. This not only protects the lens but is also easy to clean and replace.
All public transport were on hold during the pandemic. Satellite centres such as vision centres were opened after the initial phase of Lockdown was relaxed. These centres were easily approachable to patients and we used technology to connect with them through tele consultation.
Even after the public transport was restarted many elderly patients were hesitant to visit due to the fear of crowding and waiting time. We started catering to these patients through a unique idea of mobilizing the glaucoma care from hospital to their home – ‘Uberisation of Glaucoma care’. A technician fixes an appointment with the patient through the phone He carries a handheld tonometer – Icare tonometer ( has single use disposable probes) for checking intraocular pressure, non-mydriatic smartphone-based fundus photography (Remidio) for optic disc imaging and a portable head mounted virtual reality perimeter (C3FA). All the tests are done at the patient’s place and the reports are sent to the glaucoma physician who can have a teleconsultation with the patient. We are currently piloting this project and finding great results.
This pandemic has brought various challenges and opportunities to innovate new practices which can be carried forward even after the pandemic vanishes.