Join a powerful, unprecedented alliance for better eye health for all.
Join IAPBA number of conditions cause vision impairment in children such as URE, trachoma, vitamin A deficiency disorders, cataracts, and retinopathy of prematurity. Each of these require different interventions, and the prevalence of each condition varies widely amongst the regions. Data on vision impairment is often scarce and difficult to obtain for children, so it is recommended to evaluate local needs before developing a SEHP.
Uncorrected refractive errors (RE) can lead to a defocused image falling on the retina which causes blurred and/or distorted vision. Refractive errors, which are measured in dioptres (D), are the most common cause of vision impairment and can be corrected by spectacles or contact lenses in the majority of cases. There are several different types of refractive errors, each of which cause different symptoms, and occur in varying degrees in all populations. As the prevalence and types of RE vary between settings, decisions about school eye health programmes should take into account the local epidemiology of RE in school children. Information can be sought from local Ministry of Health representatives or others working in the field.
| Refractive error | Groups affected | Impact on vision/symptoms | Type of correction |
|---|---|---|---|
| Myopia | Children and adults | Clear near vision; blurred distance vision | Minus (-) spectacles or contact lenses |
| Hypermetropia/ hyperopia | Children and adults | Clear distance vision, blurred or difficulty with near vision Headaches, fatigue | Plus (+) spectacles or contact lenses |
| Astigmatism | Children and adults | Distorted vision at all distances | Cylinder (+ or -) spectacles or contact lenses |
| Anisometropia | Children and adults | Different vision impact in right and left eye | Different power spectacle lenses or contact lenses needed for each eye |
| Presbyopia | Adults aged 35-40 years and above | Difficulty seeing near objects clearly | Plus (+) spectacles |
Correcting refractive error has a positive impact on children. In fact, uncorrected refractive errors, hyperopia in particular, are often associated with poor educational performance 15-17.
Unfortunately, stigma and negative perceptions can limit spectacle wear after delivery. Health promotion activities are essential to improve compliance with wearing spectacles after screening programmes (*link to HP guidelines)
Being the most common refractive error in school-aged children, myopia can have significant impacts on children’s health and education. In fact, myopia (shortsightedness, difficulty seeing in the distance) can reduce academic performance, and increase the risk of developing vision threatening ocular complications such as retinal detachment, glaucoma and maculopathy 18. With the rising prevalence of myopia over the past decades, it has become a significant public health issue 19,20. Prevalence of myopia (with cycloplegic measurements) can reach up to 65.5% in Chinese school-children. While levels are still low in some regions such as South America and Africa, rapid urbanisation may lead to a similar shift in refractive errors 19. Many interventions are now known to delay myopia onset or reduce progression in children.
Integration of these school-based activities for myopia prevention can also have beneficial impacts on obesity rates and mental health well-being 20.
Other strategies for myopia management include optical interventions, ortho-keratology, low-dose atropine eye drops, which are proven to be more efficient to slow progression of myopia 18. However, these interventions can be very costly, require highly trained professionals and close follow-ups, which may not be possible in low-resource settings. These are not recommended as a part of a SEH program, unless proper assessment and management by trained staff are available.
The IMI Facts and Findings Infographic is a useful public health communication tool and chairside reference of key myopia management evidence-based information easily accessed by practitioners.
Strabismus (commonly known as squint) refers to misalignment of the eyes, which can shift from one eye to the other in some cases.The eye can be deviated inwards (esotropia) or outwards (exotropia), and can be constant or intermittent 24.
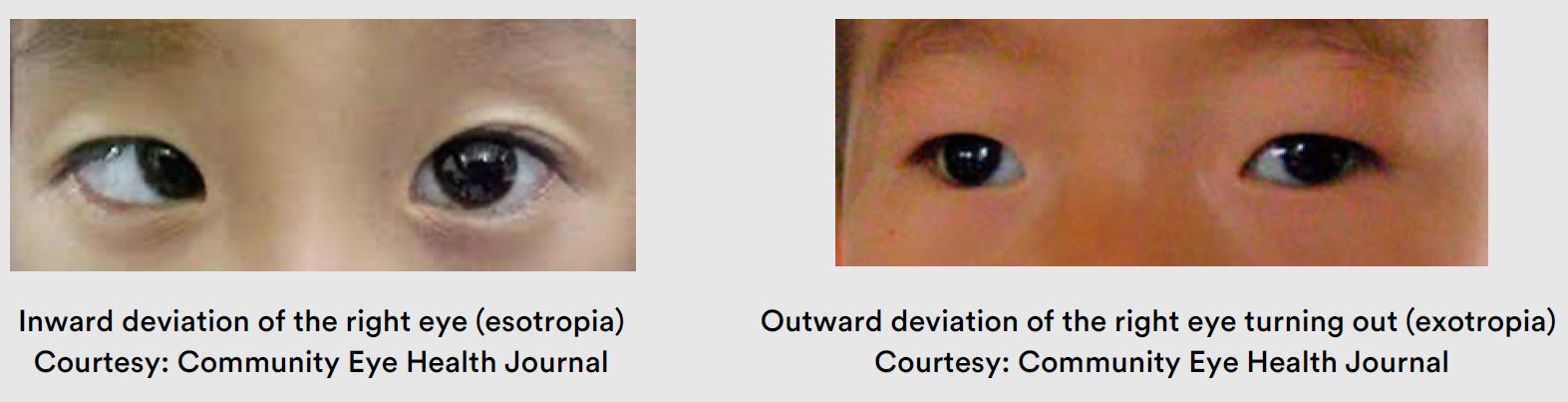
Strabismus may be present from birth (congenital), or it may develop in early childhood. In childhood the squint may be due to poor vision in one eye from uncorrected refractive error or eye conditions such as cataract or retinoblastoma. Strabismus can also occur due to problems with the muscles which move the eyes.
All children with strabismus must be referred for detailed eye examination to rule out serious underlying causes. In some cases, wearing appropriate spectacles will straighten the eyes. Other children may require surgery to realign their eyes, which can also improve their visual acuity, binocularity and appearance.
Amblyopia, or ‘lazy eye’, is one of the leading causes after refractive errors of VI in children. It can affect approximately 0.74-3.4% of children worldwide 25,26. At birth an infant’s visual system is not fully developed. Over the next few months and years, as the eyes grow, connections between the eye and brain mature, and good visual acuity is achieved for both eyes. If a clear, focused image does not fall on the retina, the development of those connections are compromised and vision is limited. This is called amblyopia, or “lazy eye”. It is most common for the vision in one eye to be affected, but occasionally both eyes can be affected depending on the cause of the visual deprivation.
| Type of amblyopia | Amblyogenic factor | Treatment |
|---|---|---|
| Refractive amblyopia | Hyperopia > 3.50D Astigmatism >1.50D Anisometropia > 1.50D | Spectacles Intermittent occlusion |
| Strabismic amblyopia | Constant tropias that are not alternating | Spectacles Intermittent occlusion Surgery |
| Visual deprivation amblyopia | Any media opacity | Surgery |
In a school-based screening, amblyopia can be detected by standard visual acuity testing of each eye, followed by refraction. If the vision does not improve with refraction, amblyopia may be the cause. Cover test, cycloplegia and ocular health assessment by trained eye care personnel can define the type of amblyopia as refractive, strabismic, organic or combined form.
The best outcomes for refractive amblyopia are seen if the uncorrected refractive error is corrected by the early age of 7 or 8 years. The vision can be improved in the lazy eye, by optical correction, intermittent occlusion (patching) of the good eye or pharmacological treatment (atropine) 27.
All children who fail vision screening in one or both eyes where refraction does not improve vision to normal in both eyes should be referred to an eye care professional for further investigation and treatment.
For more information on amblyopia: AAO Amblyopia Preferred Practice Patterns
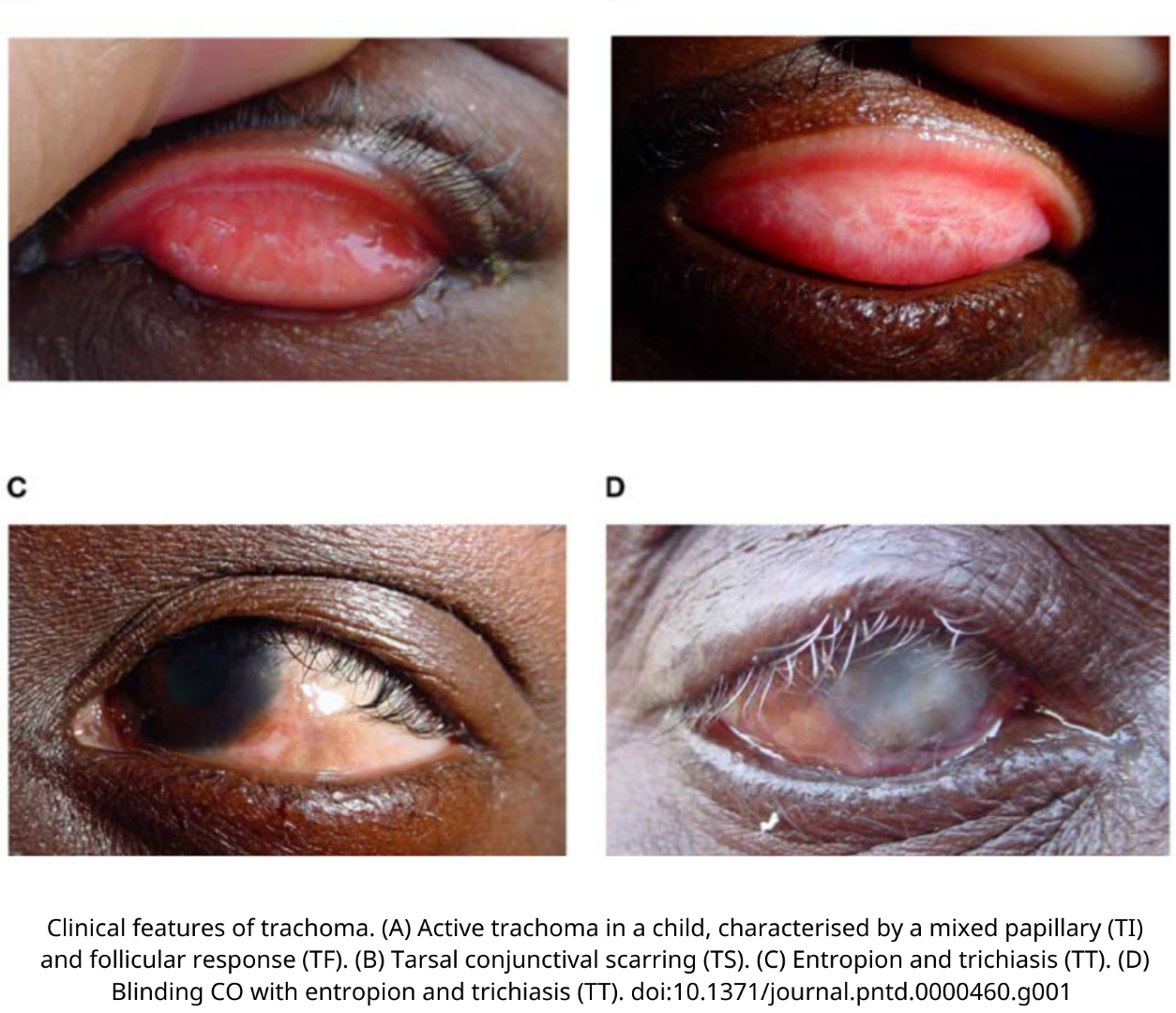
Trachoma is an ocular infection caused by chlamydia trachomatis and is the most common cause of blindness due to infectious diseases. It is transmitted by ocular and nasal secretions and principally affects the poorest communities. Public health interventions based on the SAFE strategy should be included in any school eye health programme visiting districts in which the prevalence of active trachoma is >5% in children aged 1-9 years old. Population-based surveys are indicated in districts suspected to be endemic: https://www.trachomaatlas.org
Signs of active infection such as inflammatory follicular conjunctivitis are principally found in children less than 10 years of age. The scarring stages mostly affect adults and involve the inner side of the eyelids, leading to trachomatous trichiasis (inward turning eyelashes). Left untreated, it may lead to corneal opacification and permanent vision impairment. (WHO epidemiological record 2022)
The SAFE strategy is used for trachoma control:
For more information: Trachoma Coalition
Implications for school-based screenings held in endemic regions:
Vitamin A is a crucial micronutrient for body physiologic functions. The World Health Organization estimates that 500 million children are blind due to Vitamin A deficiency disorders (VADD), with half of them dying within a year 28. It principally affects preschool children and pregnant and lactating women who live in poor communities, mostly in sub-Saharan Africa. A diet low in vitamin A rich foods, and malabsorption and diarrhoea due to poor water supplies and sanitation are the underlying causes. Children who are deficient may or may not have eye signs which are classified as night blindness, conjunctival and corneal drying (xerosis), corneal ulcers, Bitot’s spots and corneal scarring.
School health initiatives should consider addressing vitamin A deficiency disorders in all countries where the prevalence is 10% or above, particularly in schools serving rural populations.
Nutrition education, Vitamin A supplementation, food fortification and increased dietary intake can prevent vitamin A deficiency.