Join the Leading Global Eye Health Alliance.
MembershipSchool-based screenings aim primarily at detecting significant refractive errors in children and dispense glasses to those who need them. Clear criteria should be established for testing and prescription of glasses to optimise compliance and cost-efficiency of the programme. Even if WHO’s recommended distance vision indicator (eREC) is 6/12, school-based screenings should aim for a VA cut-off of 6/9 considering the excellent visual potential of children. However, a lower cut-off may lead to a higher false positive rate and therefore increase costs of the programme 5.
While myopia and astigmatism will affect distance VA, hyperopia is much more difficult to detect in a school-setting. In fact, there is no consensus yet on whether to screen children for hyperopia, but testing visual acuity with a +2.00 lens is recommended in these guidelines.
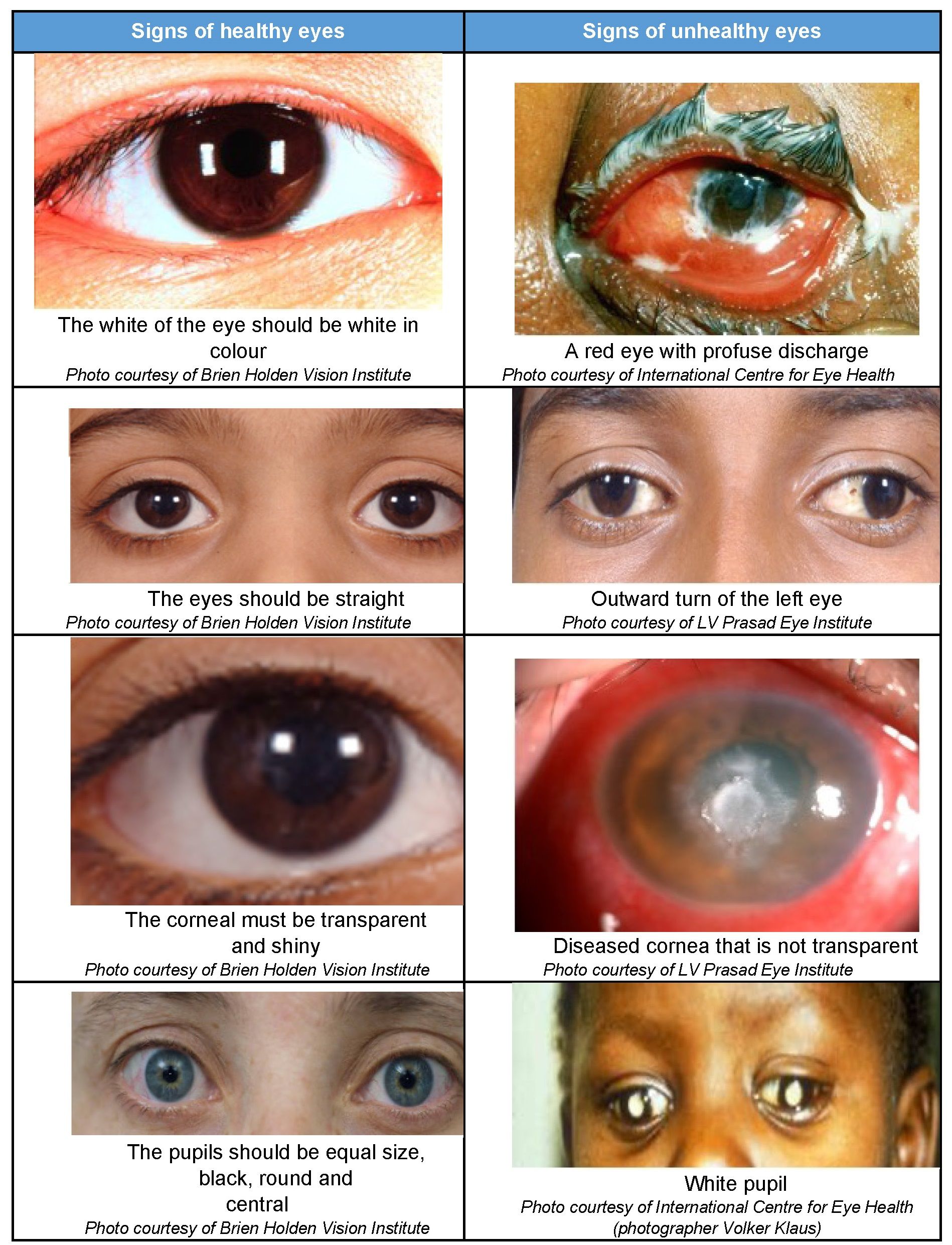
Screenings should also include identification of common eye conditions of childhood such as eye infections (conjunctivitis), lid infections (styes) and allergies (allergic conjunctivitis; vernal catarrh). Even if these conditions may not affect the visual acuity, they may keep children away from school or interfere with learning. Other more serious eye conditions which need to be detected and referred to an eye care provider for management include strabismus (in-turning or out-turning eyes), cataracts and amblyopia.