Join the Leading Global Eye Health Alliance.
MembershipA carefully planned and well organised efficient school health programme can be one of the most cost-effective investments a nation can make to simultaneously improve education and health. Integration of eye health into school health programmes is the preferred approach for the delivery of an effective school eye health programme. An effective school health program would include some awareness raising component, through community education days/sessions, in class health curriculum delivery or annual whole of school health awareness days. In addition, an effective school health program needs to include and plan clear referral approaches to ensure those children who are identified as needing follow up care can access it. Consideration should be given to exploring possibilities of bringing glasses and refractionists onsite to provide glasses on the spot for those who need them. This will increase rates of uptake and compliance. It is also crucial that a monitoring plan is included in all school health activities including data collection (both of the outputs and also costs and resource requirements) as well as some auditing of the approach to ascertain quality, further training requirements and effectiveness. An alignment between the education and health systems in implementing integrated school health programmes will work towards quality eye health services available and accessible to all children3,5,6.
In the past decades, many school eye health initiatives focused on primarily detecting distant uncorrected refractive errors in school-going children, with referral of those with other eye conditions. While this is important considering the ‘myopia pandemic’ observed in many countries, a narrow focus on refractive errors is not an efficient use of resources. It does not address non-vision impairing conditions, the eye health needs of teachers, children with other disabilities and those who are not attending school. Moreover, NGO-driven, vertical, isolated programmes that do not involve Ministries of Health or Education and are not integrated into other school health initiatives may have limited sustainability and outcomes over time.3,5,6,10
Strategies for school eye health programmes need to be comprehensive and go beyond the detection and treatment of refractive errors. It should respond to the relevant range of eye conditions and diseases prevalent in the programme area. This approach is in line with global school health initiatives such as the WHO’s “Guideline on school health services”.
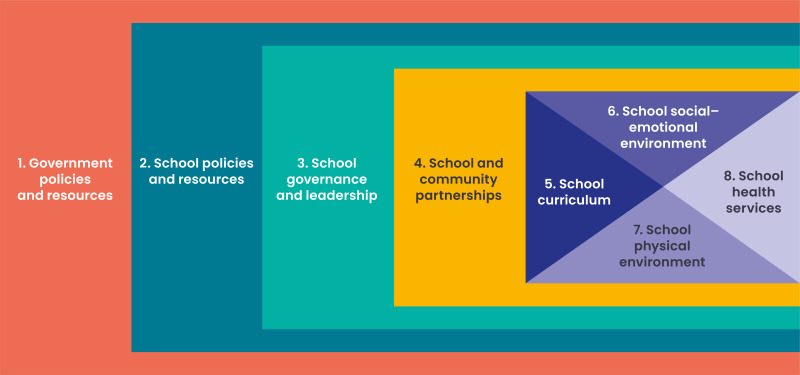
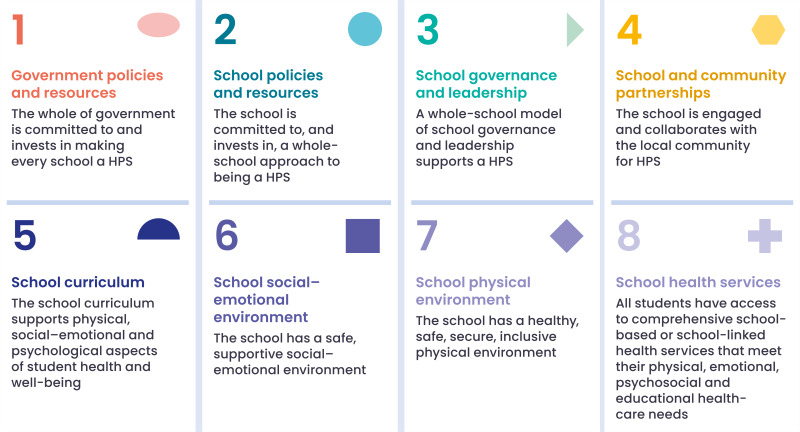
Overview of global standards for Health Promoting Schools (WHO)
Health promotion is an essential part of integrated school eye health programmes. Eye health education showed a significant increase in eye literacy 12 and may lead to better compliance13 . Eye health messages should aim to increase children’s knowledge on eye health, but should also involve parents and the whole community to reduce fears, misconceptions and social stigma on spectacle wear 5. Teachers, school administrators and school nurses are great ambassadors to integrate these messages into the school curriculum 3. Presence of parents during screenings or engaging them as volunteers have been suggested to increase eye health education and spectacle wear14.
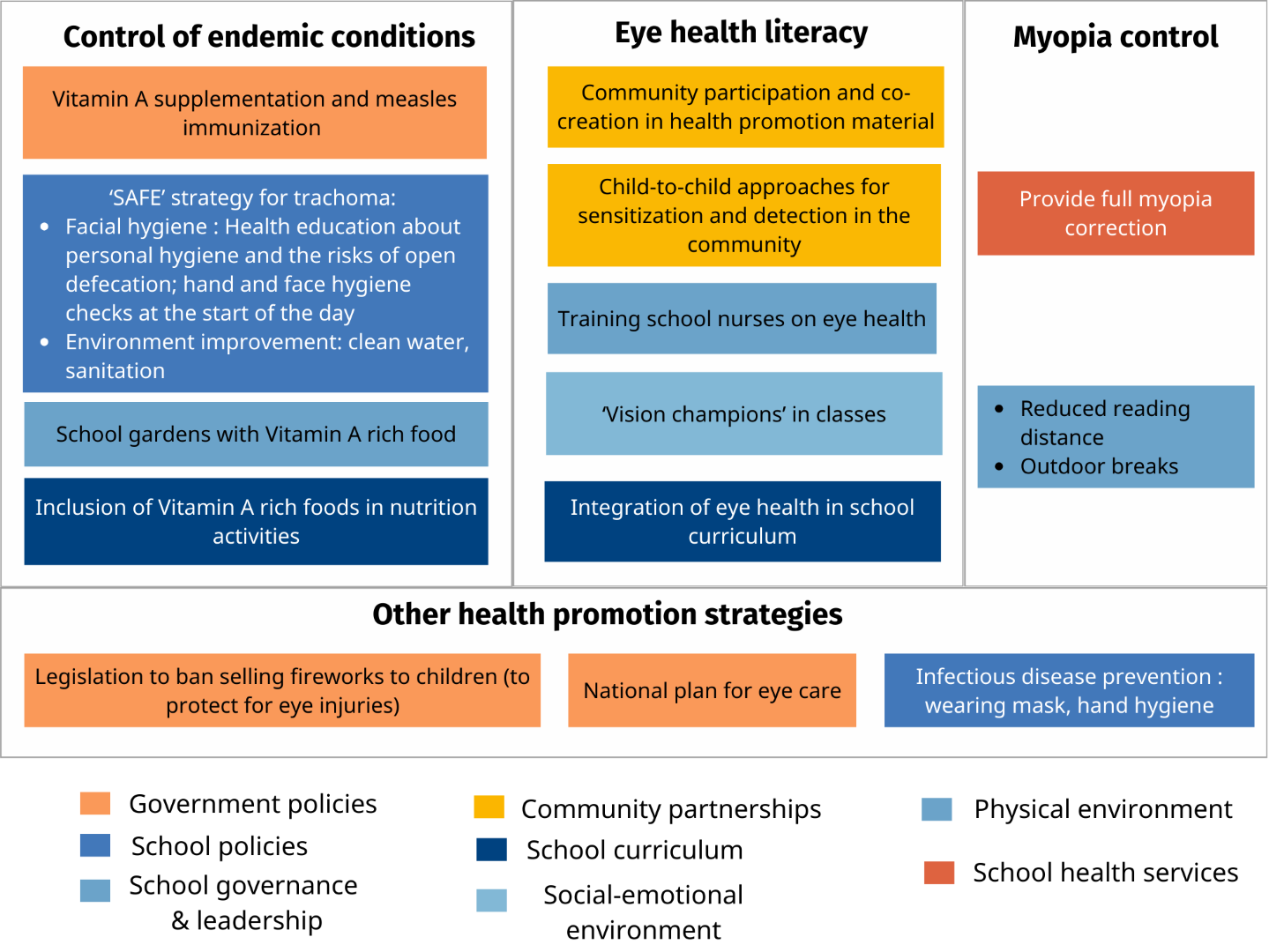
Here are some multi-level strategies that can be integrated in any SEHP depending on the conditions present in the communities. These are based on the WHO’s Health Promoting School framework 5.
In both mainland Tanzania1 and Zanzibar2, the primary obstacle to the uptake of eyeglasses was the lack of prioritization by local communities, who preferred traditional medicine as their treatment of choice. Additionally, children faced the fear of being teased by their peers as a significant barrier.3,4 Chan et al.’s5 costing analysis of the school eye health program revealed that a substantial portion (46%) of the screening kit budget was dedicated to printing information, education, and communication (IEC) materials. However, these IEC materials, including booklets, posters, and brochures, designed to engage children in Zanzibar, were negatively received and often destroyed.
In Sub-Saharan Africa, health-focused arts interventions have successfully catalyzed behavioral changes in HIV/AIDS programs and Ebola awareness campaigns.6–9 In Africa, these interventions often draw on traditional oral and performance methods, such as theater and musical approaches.10 Surprisingly, the application of arts in eye health education strategy is relatively rare. A previous arts-based, peer-delivered eyecare education intervention named Vision Champion: Children as Agents of Change11 in rural mainland Tanzania significantly enhanced the community’s eye health knowledge by 6.3%, resulting in a fourfold increase in monthly service uptake.
The success of this non-traditional intervention attracted the attention of Zanzibar health authorities, leading to the co-development of arts-based education initiatives. The Make A Difference for Vision (MAD4VISION) team started three programs: Zanzibar Arts for Children’s Eyesight (ZANZI-ACE), African Creativity for Eyesight (ACE), and Watch! Debunk! Act!
ZANZI-ACE12 focuses on traditional and contemporary musical performances in eye health education, co-created with local stakeholders. The project involved input from implementers, community members, teachers, parents, children, artists, and traditional healers to address local barriers, needs, and attitudes toward eye health. A Zanzibar-wide music competition was conducted, resulting in three selected pieces as the ZANZI-ACE eye health program intervention materials. Currently, the strategy is currently being tested in schools and communities in Zanzibar.
The ACE project takes a distinct approach by utilizing audio-visual materials, aiming to enhance relatability and effectiveness compared to the ZANZI-ACE project, which employed audio pieces. Launched in Tanzania, ACE’s package includes free-hand animation and voice drama, suitable for dissemination through social media, television, and radio, catering to diverse availability of media platforms.
The latest initiative, Watch! Debunk! Act!13, is a transformative arts and humanities project in Zanzibar. Collaborating with Tausi Women Taarab, the initiative will produce photodiaries with people with vision impairment and then transform them into two 15-minute drama videos to foster understanding and challenge and change local attitudes towards cultivating an informed, positive approach to eyecare within the Zanzibari community.
Many challenges arise when developing comprehensive SEHPs. Sustainable programmes require government ownership, involvement of multiple ministries, multi-level collaboration, stakeholder engagement, monitoring, referal pathways and long-term financing. Strong advocacy is required to prioritise eye care in most countries. Rigorous, standardised and evidence-based protocols, delivered by trained health professionals, can contribute to developing stronger and longer-lasting programmes, but access to a qualified workforce can be a significant challenge in settings where health workers are already overloaded 5.
Compliance is another major challenge for programme developers, as it is known that a high proportion of children given spectacles do not wear them. Many reasons can limit spectacle wear, from social stigma to poorly fitting spectacles 11. Education of parents, teachers and children with appropriate health literacy can help provide insight and education towards eye health 6,12. Moreover, dispensing quality spectacles only to children who really need them, and ensuring comfortable, well-fitting and cosmetically acceptable frames provided at no or minimal cost can improve educational outcomes 5. Rigorous monitoring and evaluation is essential to understand local factors influencing beliefs and limitations related to each region 11.
| Challenges | Solutions |
|---|---|
| Isolated, narrow-focused programmes | Government ownership & collaboration between ministries of Health, Education & FinanceIntegration into other school programmesPartnerships with local eye care providers (clear referral pathways) |
| Lack of standardisation | Rigorous and standardised protocols
Strong monitoring & evaluation |
| Lack of workforce | Evidence-based protocols chosen accordingly to available personnelTraining of community-level health workers as screenersLeadership, support and recurrent training for screenersContribution of teachers in health promotion & compliance |
| Lack of compliance to spectacle wear | Prescription of spectacles only when significant improvement in VA, binocularity or comfortProvision of affordable, comfortable and suitable spectacles with the right correction and quality lenses (dispensed at school where possible)Locally-developed materialParents & community participation |
| Lack of legislation for eye care providers | National guidelines on screening, eye examinations, quality of glasses & eye care plan |
| Financing | Costing of school health program to generate evidence for inclusion of eye care in national insurance schemesCross-subsidisation of services |
5,6









